Lung Health – What’s Alcohol Got To Do With It?
The effects of alcohol on the liver, heart, and brain are well known. However, the impact of alcohol on lung health is often overlooked. Our new study shows that heavy drinking may contribute to early damage in the small airways of the lungs.
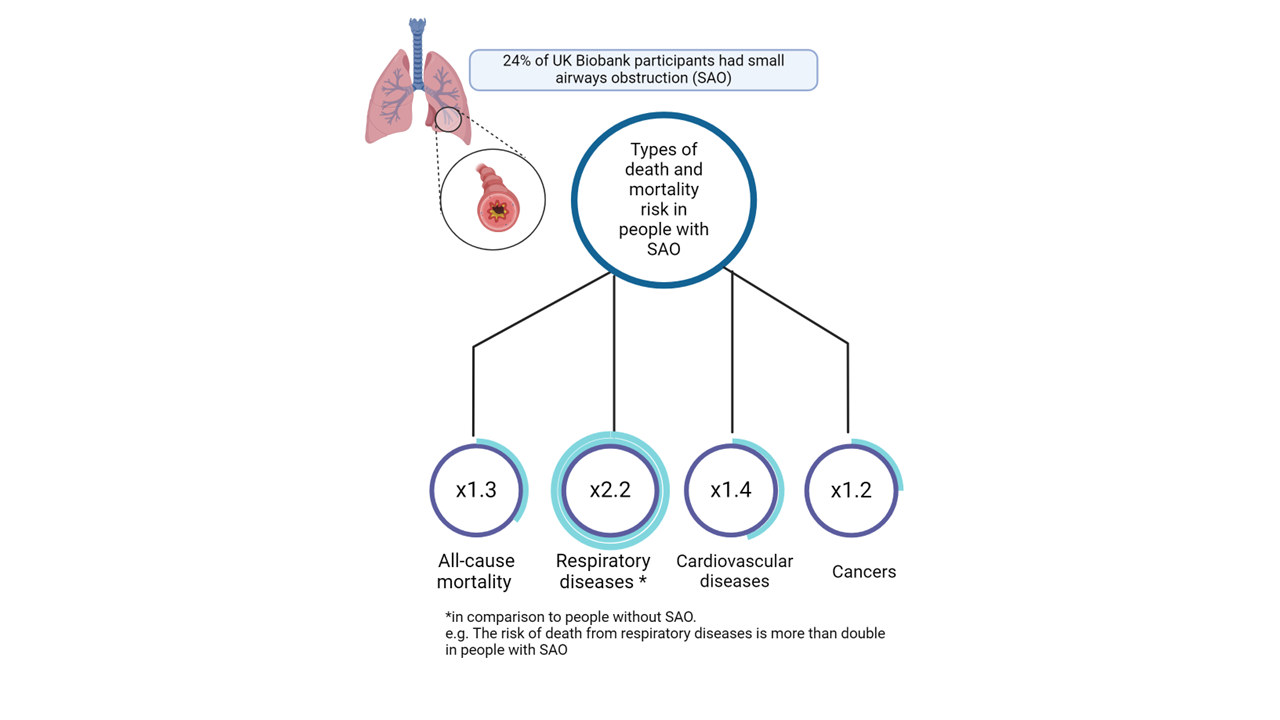
Using data from nearly 170,000 adults in the UK Biobank, we examined the relationship between weekly alcohol consumption and small airways obstruction. This condition is a subtle abnormality that can appear before asthma or chronic obstructive pulmonary disease (COPD). Because it rarely causes symptoms, this early damage is often missed in clinical settings.
After accounting for smoking, diet, socioeconomic status, and other influences, we have found that heavy drinkers were more likely to show signs of small airways obstruction than those who drink little or nothing at all. Strikingly, this association was also present among people who have never smoked, suggesting alcohol itself may contribute to early airway injury.
Moderate drinking did not significantly increase risk, but the likelihood of obstruction became clearer at very high levels of consumption. Although our findings cannot confirm causation, they add to growing evidence that alcohol may increase inflammation, weaken immune defences, and reduce the lungs’ ability to protect themselves.
These insights matter because small airways obstruction is both common and linked to the early stages of chronic lung disease. Greater awareness among clinicians and the public about alcohol’s potential role in respiratory health could support earlier prevention and intervention, complementing established risk factors like smoking.
As research continues, alcohol may deserve a more prominent place in conversations about long‑term lung health.
Check out the manuscript that has been published in CHEST and is available in open access here: https://dx.doi.org/10.1016/j.chest.2026.02.019.
 tory disease. It started with the intention to measure the prevalence, risk factors, and impact of chronic obstructive pulmonary disease (COPD) in different populations around the world. COPD is a common and serious lung condition that causes breathing difficulties, coughing, wheezing, and reduced quality of life. It is estimated that COPD affects around 300 million people worldwide and is a leading cause of death globally.
tory disease. It started with the intention to measure the prevalence, risk factors, and impact of chronic obstructive pulmonary disease (COPD) in different populations around the world. COPD is a common and serious lung condition that causes breathing difficulties, coughing, wheezing, and reduced quality of life. It is estimated that COPD affects around 300 million people worldwide and is a leading cause of death globally.