Authors: Dez Mendoza and StudentShapers Partners
Editor: Dr. Vijesh Bhute
Introduction and Scope:
“Language is an important part of the Social Model of Disability because language reflects the cultural assumptions and thinking of the society around us. Language is never purely descriptive – it shapes how we see each other, the value we place on different identities, and sometimes how we behave”. – Disability Rights UK
This document aims to provide guidance on neuro-affirmative language as well as highlighting common misconceptions with the hope to raise awareness about neurodivergent conditions. This document is created by neurodivergent students and staff.
Redefining terms:
- Neurodivergent – Describes an individual whose neurological functioning is viewed as atypical.
- Neurodivergence – The state of having a neurodivergent brain or neurotype.
- Neurodiversity – The concept that recognizes and celebrates the diversity of neurotypes across humanity. This is a natural and valuable form of human diversity.
- Neurodiverse – Refers to the natural variation of neurotypes within our society.
- Neurotypical – Someone whose neurological functioning aligns with the societal norm.
- Non-neurodivergent – A more neutral or affirming alternative to “neurotypical” that avoids centring one experience as “typical.”
- Neurodiversity-affirming – A concept that supports the view that neurodivergence is not inherently disordered but should be respected and valued. This belief celebrates the different neurotypes and focuses on neurodivergent individuals’ strengths.
- Neuro-inclusion – Describes the active and conscious creation of environments or practices designed to support and include all neurotypes. Neuro-inclusion is also the act of listening to and valuing the views and experiences.
- Neurotype – Refers to an individual’s unique neurological configuration. A neurotype covers neuro-traits and behavioural descriptors that have been grouped for diagnostic purposes. For example, autism, ADHD, dyslexia, and dyspraxia are all neuro-types under the umbrella of neurodiversity.
- Identity first language – Language that places the condition or identity before the person, which many individuals prefer. Examples include saying “autistic person” or describing someone as “dyspraxic.”
- Person first language – Language that highlights the individual before the condition. Examples include “person with autism” or “someone who has dyslexia.”
Autism
Common terms:
These are terms that may be seen in medical practice and academic or scientific literature.
- ASC – Autism spectrum condition. This term moves away from the idea that autism is a disorder. This term is more widely being used in medical settings. Note that not everyone prefers this term as calling it a ‘condition’ is a medical way of labelling and categorising.
- ASD – autism spectrum disorder. This is an outdated term which is misleading.
- Aspergers – A term that is not used anymore in the medical world. Some people may have been diagnosed with Aspergers in the past and still identify with this label. In this case, the person’s choice should be respected even if you yourself do not agree with this terminology.
- Allistic – A term that can be used to refer to someone who is not autistic.
Understanding Autism
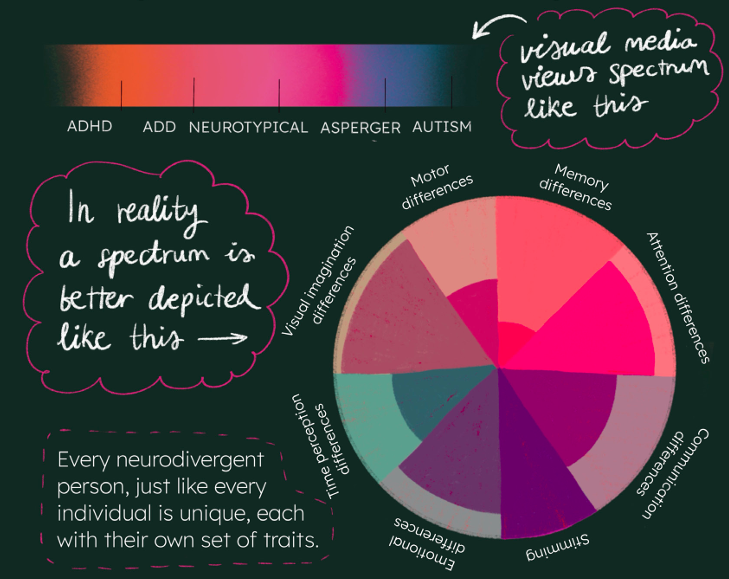
Autism varies from person to person, each person having uniquely different abilities and support needs, just as non-autistic people have varying strengths and weaknesses. Autism is not a fixed or constant state but fluctuates according to external factors or co-occurring conditions. Rather than viewing autism as ‘being on’ a [continuous or stable linear] spectrum, it may be more helpful to think of autism as being in a state of flux, or flow, subject to change, instability and inconsistency. Support needs can differ from one day to the next, or even within the same day, depending on the context of a given situation. For this reason, accommodations or adjustments need to be flexible.
It is important to consider autism or any other neurodivergence within an intersectional and cultural context. Neurotypes, which may co-exist alongside other disabilities, can present differently depending on a person’s race, ethnicity, gender identity, sexual orientation, how a person has been socialised, or class. The complex intersection of these factors can influence a person’s lived experience, resulting in discrimination or privilege.
Misconceptions
- ‘Everyone is a little bit autistic’ is a common phrase (often used by non-autistic people) when referring to what they might perceive as ‘stereotypical’ autistic traits: for example, having a specific interest or topic of conversation, or being easily annoyed or upset which might be interpreted as a ‘meltdown’. It is true that someone can have traits which may be considered autistic, but this does not necessarily mean that a person is To describe everyone as being ‘a little bit autistic’ diminishes the lived experience of autistic people and the barriers they face.
- The ‘autistic spectrum’ is often regarded as a linear form moving from less autistic (mild) to more autistic (severe) at opposite ends of the spectrum. This may lead to mislabelling of autistic people as ‘high functioning’ (mildly autistic) or ‘low functioning’ (severely autistic). Assigning these labels does not help our understanding of autistic support needs, especially if this is based on the perception of an autistic person by an external observer, rather than the autistic person’s lived experience. For example, someone who appears to be ‘high functioning’ may be ‘high masking’ – they may have low, medium, or high support needs but feel unable to advocate for their support needs because they do not want to appear difficult or demanding. This example may also be applicable to other neurotypes discussed in this document.
Inclusive/affirmative practice
When referring to a group or community:
- Use identity first language, for example, autistic person/people/community.
- Use the term ‘autism’ rather than medicalised language such as ASD, ASC, or Asperger’s.
When interacting with an individual:
- Ask whether they prefer person first or identity first language.
- Ask which terms they use to identify their neurotype(s).
- Respect their choice and use their preferred language when you are interacting with them
In addition:
- Respect the autonomy of an autistic person.
- Presume competence.
- Prioritise lived experience.
- Reframe your expectations.
ADHD
Common Terms
- ADHD: Acronym for Attention-Deficit Hyperactivity Disorder, though some individuals may reject the use of the terms “deficit” and “disorder”.
- ADD: Acronym for Attention-Deficit Disorder, an outdated term used to categorise those presenting with other symptoms of AD(H)D but lacking the “hyperactive” component. This term is now out of use and replaced with the three different models of ADHD instead.
- Attention variability/Attention rhythm/Attention difference: Centres the dynamic nature of variable attention span within individuals with ADHD, as opposed to “attention deficit”.
- Executive functions: A set of skills and functions that facilitates behaviours required to plan and execute goals. These can include self-regulation, working memory, and time management.
- Executive dysfunction: Difficulties with executive functions are a trait rather than a diagnosis. Executive dysfunction can present within several different neurotypes.
Understanding ADHD
ADHD can be categorised as Inattentive, Hyperactive, and Combined type. It is important to note that a spectrum of ADHD symptoms can exist across the different types, and just because two individuals have the same type of ADHD, does not mean that the two individuals experiences ADHD the same way.
Misconceptions
There is a common misunderstanding by the wider community that ADHD presents as the stereotypical “hyperactive child with the inability to sit still”. This is not only harmful by reducing ADHD presentation and types to one singular presentation but also can often lead to under-diagnosis within assigned female at birth (AFAB) and other minority communities. ADHD presentation can often differ due to cultural and societal differences.
- ADHD isn’t just someone not sitting still, therefore hyperactivity may not be the only indicating factor of diagnosis
- Due to societal expectations, girls and AFAB children are often underdiagnosed when they don’t exhibit the hyperactivity stereotype.
- Executive dysfunction — often misconstrued as “laziness” or simple procrastination, executive dysfunction can significantly impair a person’s ability to plan, initiate, organize, and complete tasks, even when they are motivated and aware of what needs to be done.
Another common assumption of ADHD is the view that it is a “childhood disorder”. ADHD has been seen to carry into adult life, and societal pressure often causes individuals to conform to neurotypical social practices, also known as “masking”, to alleviate stigma associated with ADHD behaviour.
Inclusive/affirmative practice
When referring to a group or community:
- Both identify first (e.g. “ADHD-er” or “ADHD community”) and person first (e.g. “person with ADHD”) are widely accepted.
When interacting with an individual:
- Ask whether they prefer person first or identity first language.
- Ask which terms they use to identify their neurotype(s).
- Respect their choice and use their preferred language when you are interacting with them.
Dyslexia
Common terms
These are terms that may be seen in medical practice and academic or scientific literature; however, this is not always the most affirming language.
- Dyslexia – A condition that affects how the brain processes written and spoken language.
- Dyslexic thinking – Reframes dyslexia not as a deficit, but as a distinct and valuable cognitive style. Focuses on the ability to recognise patterns and problem solve.
- Learning difficulty – Refers to specific challenges in acquiring academic skills (e.g. dyslexia, dyscalculia). Does not affect general intelligence.
- Learning difference – A broader, more inclusive term that acknowledges diverse ways of learning.
- SpLD – Specific learning difficulty. Encompasses several different learning difficulties.
- SLD – Specific learning disability. More commonly used in a medical and legal contexts.
Understanding Dyslexia
Dyslexia is a specific learning difference which affects information processing speed in the brain. Dyslexia can make it difficult to structure thoughts and sentences. Dyslexic individuals can present with difficulties related to memory, planning, time management, and directions (left/right, etc). Dyslexic individuals are also known to have improved problem solving and creative thinking skills. It is important to note that this is not an exhaustive list of traits and not everyone presents with all traits. Additionally, dyslexia may be considered a disability by some individuals while others may prefer to refer to it as a learning difference.
Misconceptions
- Dyslexia is just reading and writing challenges – this is not true. As discussed above dyslexia can affect other aspects of information processing including memory, planning and structuring thoughts. Not all dyslexic individuals have writing difficulties.
- Dyslexia can be outgrown. This is incorrect – dyslexia is a lifelong condition, but with appropriate support and strategies, individuals can learn to manage it effectively.
- Dyslexia is just about reversing letters. Again, this is a misconception: while letter reversal is a symptom, dyslexia primarily affects reading fluency and comprehension.
Inclusive/affirmative practice
- On a community and individual level: “dyslexic individual(s)” or “individual(s) with dyslexia”.
- It is very important to keep intersectionality in mind to avoid misunderstanding someone’s support needs.
- It is also vital to keep in mind that everyone’s dyslexia symptoms will be different and different dyslexic individuals might require vastly different support.
Dyspraxia
Common terms
- Developmental co-ordination disorder (DCD): This term is seen in medical practice and academic or scientific literature, but dyspraxia is the preferred term.
Understanding Dyspraxia
Dyspraxia is a difference that affects movement and co-ordination. It does not affect one’s intelligence. It can affect one’s co-ordination (large motor) skills, such as tasks requiring balance, playing sports, or learning to drive a car. Dyspraxia can also affect fine motor skills, such as writing or using small objects. The degree of impact on large and fine motor skills varies between individuals.
Misconceptions
- Dyspraxia is just being clumsy – Dyspraxia affects motor coordination, but it also impacts planning, organization, memory, speech, and emotional regulation. It’s a neurological condition, not simply clumsiness.
- Dyspraxia only affects coordination – It can also affect fine motor skills, speech and language development, sensory processing, and even social interaction and emotional wellbeing.
- Children outgrow dyspraxia – Dyspraxia is a lifelong condition. While some individuals may develop coping strategies or improve certain skills over time, the underlying neurological differences remain into adulthood.
Inclusive/affirmative practice
When referring to a group or community:
- Use identity first language, for example dyspraxic person/people/community.
- Use the term ‘dyspraxic’ rather than medicalised language such as DCD.
When interacting with an individual:
- Ask whether they prefer person first or identity first language.
- Ask which terms they use to identify their neurotype(s).
- Respect their choice and use their preferred language when you are interacting with them.
The neurodivergent umbrella
The 4 conditions outlined above are some of the most common and well-known neurotypes. There are, in fact, several other neurotypes that fall under the neurodivergent umbrella. This includes conditions such as:
- Dyscalculia
- Dysgraphia
- Tourette’s syndrome
- Sensory processing disorder
- PTSD and c-PTSD ((complex-) post-traumatic stress disorder)
- OCD (obsessive compulsive disorder)
- Bipolar
- Down’s syndrome
- Foetal alcohol syndrome disorder
- Epilepsy
In the international context of Imperial, it is worth to keep in mind that some students come from countries and families where neurodivergence is highly stigmatised. They therefore may not know which adjustments are available and what would be helpful to them. The journey of discovering this for themselves is especially confusing in such an intense and fast paced environment as university in a new country.
Further reading
- Bhute, Vijesh; Cracknell, Maya (2026). Neurodiversity at University.
- Eight principles of neuro-inclusion; an autistic perspective on innovating inclusive research methods
- Why ‘Neurodiversity’ and ‘Neurodivergence’ Shouldn’t Be Used Interchangeably | The Swaddle
- Neurodiversity affirming care-what does it mean for therapy?
- An Event Professional’s Guide to Neuroinclusion
- Top tips for Neuroinclusive communication | John Innes Centre
- Voices of neurodiversity | Chris Papadopoulos
- We’re all neurodiverse | Sonny Jane Wise
- ‘It’s like calling short people vertically challenged’: Language and terminology preferences among neurodivergent adults in the United Kingdom – Amy Pearson, Aimee Grant, Jennifer Leigh, Stephen J Macdonald, Kathryn Williams, Gemma Williams, Elliott Spaeth, Kieran Rose, Ann Memmott, Monique Botha, 2026
This resource is part of the Inclusive assessments project funded by the Pedagogy Transformation Fund at Imperial College London. For any questions or comments, please contact Dr. Vijesh Bhute (v.bhute@imperial.ac.uk).
