HIV Co-Production


On Wednesday 6 July 2022, 25 stakeholders met at Lift, Islington (a community venue) to reflect, create and share ideas together as a group about co-producing HIV research using the example of a recent participatory project exploring the impact of COVID-19 on people living with HIV in the UK
The showcase event was co-designed to be interactive and participatory in nature (after all, we wanted to showcase how valuable these approaches can be to research!). You can find out more about how we co-designed the day in our previous blog.
The day started with an icebreaker over a networking lunch – we chose “human bingo” where each person is given a card (see picture below) and asked to find someone in the room who corresponds to a statement on the card. We opted for a mixture of “research related” and more informal statements which would act as conversation starters and would also help attendees to get a sense of who else was in the room.

After lunch and the icebreaker, we then moved on to presentations on our participatory research project approach, findings and reflections alongside more creative activities.
Drawing concepts – what does co-research mean to you?
The activity was designed to get people to meet others on their table and get them talking. We asked each table to discuss and draw “what co-research means to you”. Each table was then asked to present back their ideas in 60 seconds. We adapted this activity based on the IIED Participatory Learning and Action Trainer’s Guide (Pretty et al., 1995; p139)
We heard a range of descriptions about what co-research meant to them across the groups, including.
Co-research means:
- Diversity, meaningful involvement and participation – everyone is able to participate in a way where power is shared/disrupted
- Although this is influenced by the current structure of research funding and it is not always easy to have equal power) – equality.
- Power sharing is also difficult and messy – you need to be invested but it results in larger impact (a “level playing field”)
- Working/designing with others in partnership & building networks and relationships including those outside your comfort zone
- All stakeholders (private, public, voluntary) working together towards a specific goal and shared decision making at each stage of the research cycle (from designing the research question to disseminating the findings). There is “power in numbers”
- Learning from each other in a consultative/iterative process (designing and re-designing)
- Communication including simplicity, well-moderated discussions and active listening
- Trust, respect and honesty
- Warmth and rapport
- Generating knowledge and skills building in a way that challenges the norms of research by “questioning who is the expert”
- Co-production is as valid as traditional research approaches and can produce quality research findings
- Community-driven outcomes and solutions which are ultimately impactful to the community
- Awareness in the community
- Feedback-loop with the community
- Sharing results “in the right way, to the right people”
- Acknowledging and recognising contributions –ideas incorporated in the research process which will empower and motivate those involved.
One group also reflected on whether “research without co-production can succeed?” They defined “success” as making a change.

Discussion and priority setting – so what? Now what?
After presenting our preliminary research findings, we undertook a nominal group technique with each group. Nominal group technique is a structured method for group brainstorming that encourages contributions from everyone and fosters quick agreement across stakeholders on the most important issues.
This session was facilitated by staff/co-researchers and asked each group to discuss which results we should prioritise sharing and who we should be sharing these will, as well as the most important recommendations for potential changes to policy and services following from our findings.
We adapted this activity based on the IIED Participatory Learning and Action Trainer’s Guide (Pretty et al., 1995; p157-158)
This activity was split into two sections (we had a well-earned break in between!) and involved:
- Silent idea generation (~ 5 mins) – each person writes possible solutions on their own on a piece of card/paper
- Round-robin reporting of ideas (~10 mins) – each person shares their ideas one at a time to the table. The facilitator writes in people’s exact words until everyone has shared as many as they want. Each idea is labelled with a letter of the alphabet.
- Discussion for clarification (~10 mins) – open discussion to clarify ideas (e.g., meanings of words, phrases etc.)
- Ranking according to importance (~10 mins): each person records 5 items (1 per card) of highest priority from those on group flipchart. Each member identifies and ranks from 5 (highest) to 1 (lowest priority). All cards collected and tallied on master sheet
Overall, issues around mental health and inequalities including the provision and structure of services were identified as key priority areas. On each of the tables, the ideas which were considered the highest priority were:
- Early intervention for mental health – better awareness of mental health issues and where you can get help. More availability and ability to access mental health services through early intervention.
- Access to GP/care needs to adjust to address issues with mental health (service adaptation)
- Increased messaging around mental health and HIV (health promotion)
- Louder patient voice and choice in how services are provided (service provision) – particularly around issues of loss of body language in remote consultations
- Influencing integrated care systems
- Mental health and wellbeing to be fed back to providers and commissioners – isolation and loneliness does not just affect people with HIV
- Inequality in accessing healthcare due to digital/gadget poverty
- How to build into services the support for people who are living in increased poverty
- Will annual blood tests reduce confidence in U=U
- Equality of access to services in the UK
Group collages – the principles of co-production
Our final activity of the day was the most creative yet (!) it involved each table creating a collage on a principle of co-production using magazines, newspapers and flyers. These principles were selected from our previous work with the NIHR ARC NWL, IGHI and Heart n Soul and were presented at both the NCRM eFestival 2021 (more here) and Imperial College Engagement Day 2022.
Each table was asked to move to another collage after 10 minutes to allow them time to contribute ideas on each co-production principle collage (below).
Panel discussion, reflections, and feedback
We finished the day with a panel discussion featuring our co-researchers (Silivia, Husseina and Wezi) and academic staff (Vas, Halle and Jane). We reflected on our experiences working together, sharing power and our hopes for the future of co-production.
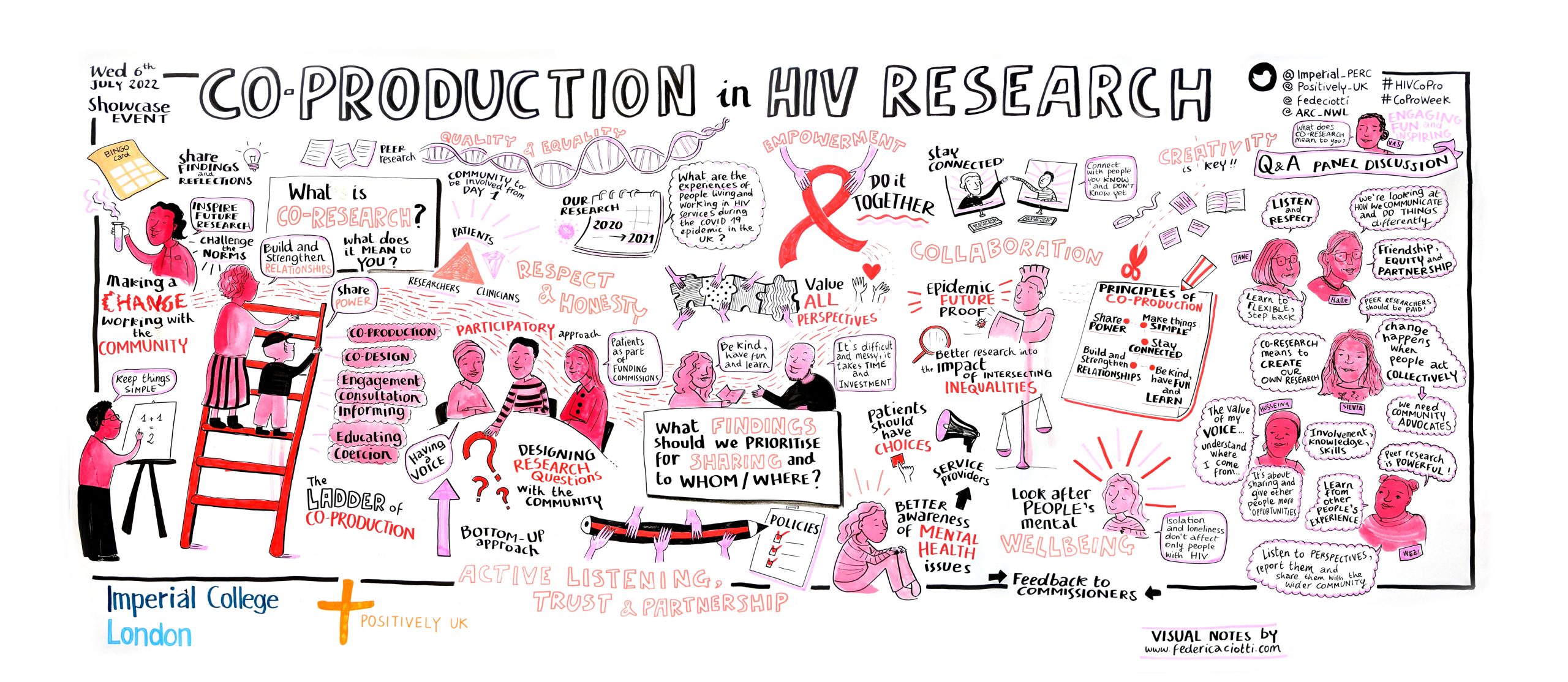
Our discussion across the event, was also captured throughout the day (located at the top of the blog) by our visual notetaker Federica
We also encouraged everyone to add their thoughts, ideas and feedback to our “feedback wall” which was inspired by the work of our colleague Kelly Gleason. The feedback from the event was extremely positive, with attendees saying
‘Great to see peer research done well and honouring the spirit of co-production’
‘Good to meet such a friendly group of people sharing common goals’
‘An amazing afternoon, thank you! Wonderful to see peers having so much agency over where research is moving’
‘Loved the creativity’
Finally, we are excited to showcase our video which was created following the event by our fantastic filmmaker, Ed Rolfe, and features several of the team sharing their reflections of working together and co-production.
This event, and all our work so far, has been a huge learning curve for the team. We have learned the art of keeping things simple and how co-production, when done properly and in a respectful way, can really help to make research more accessible to everyone. We have built friendships with our co-researchers and can’t wait to see what the future holds for both the project and our co-researchers!
We’d also like to give a huge thanks to those who attended our event and participated throughout the day as well as the funding received from the Societal Engagement Team’s Participatory Research Fund.
For more on our work so far and for future updates please visit our project webpage
If you would like further information about the study or have any questions, please contact Vas at vasiliki.papageorgiou17@imperial.ac.uk or @vaspapa_
This blog was co-authored by members of the project team (left).
Note: This work is one part of a wider project exploring experiences of the COVID-19 pandemic from HIV clinical- and community-based workers and volunteers (you can find out more about the other parts of this study here). It also feeds into a larger doctoral research project (using the 2017 Positive Voices survey data) looking to explore the impact of social determinants (e.g. housing, employment, income etc.) on the health and wellbeing of people living with HIV.
This work is funded by Imperial College London’s Societal Engagement team 2020 Rapid Response Seed Fund and Participatory Research Seed Fund and supported by an ESRC LISS Doctoral Training Partnership (DTP). The work would not have been possible without the generous support and time of our co-researchers and study participants.