Despite the very low risk of seroconversion, occupational HIV exposure is a very stressful situation. Our new article in the Journal of the Royal Society of Medicine provides guidance on how such exposures should be managed to minimise risks and improve health outcomes for staff exposed to contaminated body fluids.
Careful risk communication can help in addressing anxiety. Pre-Exposure Prophylaxis (PEP) is seldom indicated for occupational exposures if the index case is of unknown HIV status, as the transmission risk is very low. PEP is indicated to reduce the transmission risk following high-risk incidents – exposures where the index case is known to be HIV-positive with a detectable viral load – and is most effective if started promptly.
One of the causes of increased workload in general practice are the many requests that doctors get for letters from patients or from external organisations. It’s now so common that doctors have coined a term for it: GANFYD – Get A Note From Your Doctor.
It’s seems that large sections of society can’t function without these “letters from doctors”. Instead of using common sense or employing their own clinical advisers, external organisations make repeated requests to NHS doctors for letters which are not at all needed.
Often the worst offenders come from the public sector – e.g. universities who seem to look upon NHS general practice as a source of free occupational health advice for their students. Universities never – of course – offer to pay for this advice they get from NHS GPs.
Instead, university requests will come with a mealy-mouthed statement that any fee is the responsibility of the student. Like doctors are going to impose heavy fees on impoverished students who already have large debts and are who are often living in poverty.
Local government and schools are other frequent offenders, requesting letters for issues they could easily resolve themselves using some common sense. And perhaps surprisingly, the NHS is also a frequent offender (you would think that NHS Trusts would know better).
What’s the solution? I have concluded that to address the GANFYD problem, we need to remember the adage “money talks while bullshit walks”. But don’t charge patients. Change NHS regulations so the (suitably large fee) is the responsibility of the organisation making the request.
The NHS is under great pressure and we urgently need to do everything we can to reduce unnecessary work in the NHS so that NHS staff can focus on clinical work.
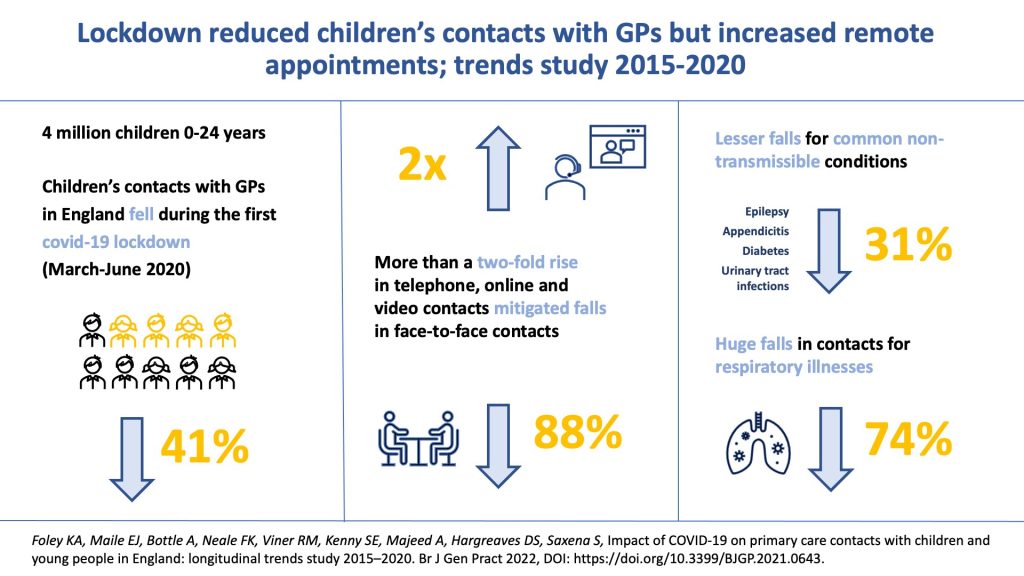
During the COVID-19 pandemic, health systems globally shifted towards treating COVID-19 infection in adults and minimising use of health services for other patients, including children and young people (CYP), who were less susceptible to severe COVID-19. In March 2020, the NHS recommended remote triaging before any face-to-face contact to reduce infection risk.
The UK Government announced a nationwide lockdown in England from 23 March 2020, and the public was advised to stay at home to limit transmission of COVID-19 and avoid strain on health resources. GPs were asked to prioritise consultations for urgent and serious conditions, and suspend routine appointments for planned or preventive care.
Children’s access to primary care is highly sensitive to health system changes. We examined the impact of COVID-19 on GP contacts with children and young people (CYP) in England. We used a longitudinal trends analysis was undertaken using electronic health records from the Clinical Practice Research Datalink (CPRD) database.
GP contacts fell 41% during the first lockdown compared with previous years. Children aged 1–14 years had greater falls in total contacts (≥50%) compared with infants and those aged 15–24 years. Face-to-face contacts fell by 88%, with the greatest falls occurring among children aged 1–14 years (>90%). Remote contacts more than doubled, increasing most in infants (over 2.5-fold). Total contacts for respiratory illnesses fell by 74% whereas contacts for common non-transmissible conditions shifted largely to remote contacts, mitigating the total fall (31%).
In conclusion, CYP’s contact with GPs fell, particularly for face-to-face assessments. This may be explained by a lower incidence of respiratory illnesses because of fewer social contacts; changing health-seeking behaviour; or a combination of both. The large shift to remote contacts mitigated total falls in contacts for some age groups and for common non-transmissible conditions.
Recent draft guidance from NICE gives a much bigger role to exercise and weight loss in people with osteoarthritis, and painkillers such as paracetamol and strong opioids not advised.
I agree that the aims of the new draft NICE guidance on the management of osteoarthritis in primary care are good but the problem will be in providing patients with access to suitable lifestyle and exercise programmes. In many parts of England, these services are either not currently in place or have very limited capacity. As well as putting in place services with sufficient capacity, we also need to ensure there is equitable access to them, based on clinical need. We know from prior experience that it is more affluent and better educated patients who are more likely to take up these kind of lifestyle and exercise interventions.
We also need to simplify clinical pathways and allow patients to refer themselves directly to services without requiring a referral from a GP. This will improve the speed of access to these services for patients and reduce the demands on already over-stretched GP services.