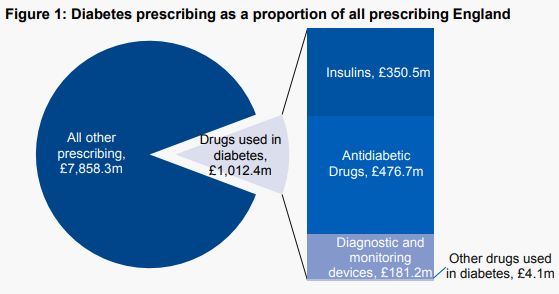
 Drugs used to treat diabetes are now responsible for 11.4% of total primary care prescribing costs in England, £1,012 million annually. The very high costs to the NHS of treating diabetes are an inevitable consequence of the increase in the prevalence of type 2 diabetes in recent decades. This increase in the prevalence of type 2 diabetes is in turn a consequence of lifestyle factors such as high-calorie diets (particularly diets high in sugars and refined carbohydrates), physical inactivity and obesity. We need effective strategies at both population and individual level, and changes in the obesogenic environment we live in, to reverse these adverse lifestyle- associated factors and bring down the prevalence of type 2 diabetes.
Drugs used to treat diabetes are now responsible for 11.4% of total primary care prescribing costs in England, £1,012 million annually. The very high costs to the NHS of treating diabetes are an inevitable consequence of the increase in the prevalence of type 2 diabetes in recent decades. This increase in the prevalence of type 2 diabetes is in turn a consequence of lifestyle factors such as high-calorie diets (particularly diets high in sugars and refined carbohydrates), physical inactivity and obesity. We need effective strategies at both population and individual level, and changes in the obesogenic environment we live in, to reverse these adverse lifestyle- associated factors and bring down the prevalence of type 2 diabetes.In an article published in the British Medical Journal, I discuss the health outcomes achieved by the NHS in the UK and how these compare with other European countries. Health outcomes in the UK have improved substantially since the NHS was established in 1948. The NHS also performs well in many international comparisons on measures such as efficiency, equity, and access.
Despite these achievements, however, problems with health outcomes remain. Moreover, other European countries have also improved their health outcomes in recent decades, often at a faster rate than the UK. Consequently, the UK now lags behind many other European countries in key health outcomes in areas such as child health and cancer survival.
I conclude that new health policies in the UK should help the NHS to focus on improving health outcomes and that politically expedient schemes that are not evidence-based – such as extended opening hours in primary care – should be abandoned. Continued progress is also needed on wider determinants of health such as poverty, housing, education, employment, and the environment.