Please note that I made these for my own use but thought they may be useful to others!
Cardiac Pathology
Divided into diseases of the:
- Coronary arteries
- Endocardium (including valves)
- Myocardium (including congenital heart disease)
- Pericardium
- Coronary arteries
Any vascular disease can involve these (e.g. vasculitis) but atheroma is the important one.
Clinically: angina, unstable angina and myocardial infarction (due to superimposed thrombosis secondary to ulceration or fissuring).
Left coronary artery >
- anterior descending > anterior septum and wall of left ventricle
- circumflex branch > lateral wall of left ventricle
Right coronary artery > posterior septum and wall of left ventricle
Distribution of infarction:
- Subendocardial infarction due to severe, generalized disease.
- Focal due to blockage of a major artery.
Complications of myocardial infraction:
Minutes:
Arrhythmias: ventricular fibrillation / heart block
Acute cardiac failure / cardiogenic shock
Days:
Thromboses:
- Mural (over the infract) which may be followed by systemic embolisation
- Atrial thrombus (due to atrial fibrillation)
- (DVT which may be followed by pulmonary embolization)
Week:
Rupture (due to softening of muscle):
- Myocardium (leading to cardiac tamponade and death)
- Papillary muscle (mitral incompetence)
- Septum (left to right shunt)
Pericarditis
Weeks:
- Chronic cardiac failure.
- Immune pericarditis (Desslers’s syndrome)
Months:
Cardiac aneurysm (due to fibrosis)
At any time:
Another infarct
- B) Myocardium
Myocarditis
Causes:
Infectious:
- Viral e.g. Coxsackie
- Bacterial e.g. Borrelia (Lyme Disease)
Toxic: e.g. Diphtheria
Immunological e.g. Rheumatic fever
Cardiomyopathy:
Definition: Heart muscle disease not due to ischaemia, hypertension, valvular disease or inflammation
- Dilated cardiomyopathy: end stage of the above (which has burnt out), alcohol or pregnancy
- Hypertrophic cardiomyopathy: autosomal dominant
- Restrictive cardiomyopathy: endomyocardial, fibro-elastosis, amyloid, haemochromtosis
Rheumatic fever
Preceded by streptococcal sore throat.
Type 2 hypersensitivity reaction (antibodies to streptococci cross react with antibodies to myocardium.
Clinical features
- General: fever etc.
- Skin: nodules
- CNS: chorea
- Heart:
- Pericarditis
- Myocarditis (Aschoff bodies- collections of macrophages)
- Endocarditis including valves – may lead to chronic valve disease (see below)
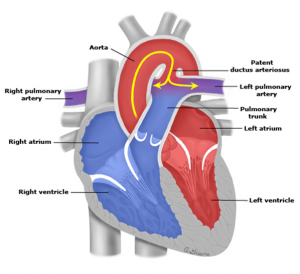
Congenital Heart Disease
Risk factors: e.g. Down’s syndrome, rubella, thalidomide
- Left to right shunts e.g. atrial or ventricular septal defects ( if untreated may reverse
- Right to left shunt “ Cyanotic”
e.g. Tetralogy of Fallot:
- large ventricular septal defect
- pulmonary stenosis
3) overriding of the aorta
4) right ventricular hypertrophy
- C) Endocardium
Valve disease
Mitral valve:
Leads to dilation and hypertrophy of the left atrium
In incompetence there is, also, dilatation of the left ventricle
Incompetence:
- Post -inflammation: rheumatic fever
- Infective endocarditis
- Left ventricular failure
- Myocardial infarction
- “Floppy mitral valve syndrome”
Stenosis:
- Post-inflammation: rheumatic fever
Complications:
- Atrial fibrillation
- Infective endocarditis
Aortic valve:
Stenosis:
- Age related calcification
- Calcification of abnormal valve:
Congenital bicuspid
Post -inflammation: rheumatic fever
Leads to marked cardiac hypertrophy and the risk of sudden death
Incompetence
- Post -inflammation: rheumatic fever
- Infective endocarditis
- Dilatation of valve ring e.g. Marfan’s syndrome
Leads to dilatation and hypertrophy
Infective endocarditis
Vegetations form on the valves
- Acute:
Pathogenic organism (e.g. staphylococcus aureus) and normal valve
- Subacute:
Less pathogenic organism (e.g. streptococcus viridans, from the mouth, or enterococci, from the gut) and an abnormal valve
Complications:
- Systemic features: Fever etc.
- Embolisation of vegetations
Infected infarcts in the brain or kidneys
Splinter haemorrhages
Other causes of valve vegetations
e.g. marantic in patients with cancer
- D) Pericardium
Classified according to appearance
- Fibrinous e.g. myocardial infarction
- Serous e.g. rheumatic fever
- Purulent e.g. bacterial infection
- Haemorrhagic e.g. traumatic, tumour
- Fibrotic +/- calcification (chronic) = constrictive pericarditis g. TB
Pericardial haemorrhage:
- Myocardial infarction
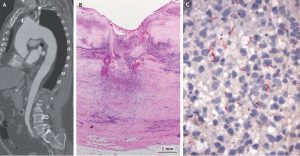
- Dissecting aortic aneurysm
Read Some Notes on Cardiac Pathology in full