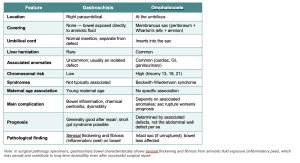
A newborn presents with choking, coughing, and vomiting after taking the first feed. The nasogastric tube has passed but coils in the upper oesophagus.
The most likely diagnosis is oesophageal atresia, which is usually associated with a tracheoesophageal fistula.
Atresia, stenosis, fistulae, and duplications
These can occur anywhere in the gastrointestinal tract.
- Atresia is when there is a thin, non-canalised cord-like structure that replaces the normal structure.
- Stenosis is when the bowel is markedly narrowed. These are most clinically significant in the oesophagus and small intestine because of their relatively narrow lumen.
- A fistula is an abnormal communication between two epithelial-lined surfaces. The oesophagus and the trachea or bronchus in the examples below.
- Duplications are segments of the bowel that are duplicated!
Oesophageal atresia,
In the context of the oesophagus, atresia is very frequently associated with a tracheoesophageal fistula (and vice versa). There are a number of possibilities, with type C being the commonest.
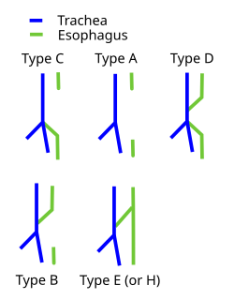
en.wikipedia.org/…/Tracheoesophageal_fistula
Because there is a complete obstruction in the oesophagus immediately after birth, there are symptoms such as choking, coughing, and vomiting as a result of the obstruction, regurgitation and aspiration.
It should be noted that before birth, oesophageal atresia is associated with oligohydramnios
When an attempt is made to pass an oesophageal probe, it will not pass due to complete obstruction, which can be demonstrated on imaging.
Treatment is urgent surgery.
As usual, it is important to remember that once a congenital abnormality is present, there are likely to be others. Oesophageal atresia is, e.g., associated with an increased risk of imperforate anus.
In addition to atresia, congenital stenosis can occur. Other causes (in adults) of oesophageal stenosis include: gastroesophageal reflux, swallowing sodium hydroxide, radiation or scleroderma. Scleroderma and radiation also cause fibrosis in the lungs and heart (leading to cardiomyopathy).
Robbins: page 685.
Read GI: Paedatric Pathology Case 1 in full